MR Online | Why Is Cuba’s Health Care System the Best Model for Poor Countries?
MR Online | Why Is Cuba’s Health Care System the Best Model for Poor Countries?
Why Is Cuba’s Health Care System the Best Model for Poor Countries?
Posted Dec 07, 2012 by Don Fitz
Topics: Climate Change , Ecology , Health
Places: Cuba , Ghana , Haiti , Latin America , Pakistan , Peru , Ukraine , Venezuela
Furious though it may be, the current debate over health care in the US is largely irrelevant to charting a path for poor countries of Africa, Latin America, Asia, and the Pacific Islands. That is because the US squanders perhaps 10 to 20 times what is needed for a good, affordable medical system. The waste is far more than 30% overhead by private insurance companies. It includes an enormous amount of over-treatment, creation of illnesses, exposure to contagion through over-hospitalization, disease-focused instead of prevention-focused research, and making the poor sicker by refusing them treatment.1
Poor countries simply cannot afford such a health system. Well over 100 countries are looking to the example of Cuba, which has the same 78-year life expectancy of the US while spending 4% per person annually of what the US does.2
The most revolutionary idea of the Cuban system is doctors living in the neighborhoods they serve. A doctor-nurse team are part of the community and know their patients well because they live at (or near) the consultorio (doctor’s office) where they work. Consultorios are backed up by policlínicos which provide services during off-hours and offer a wide variety of specialists. Policlínicos coordinate community health delivery and link nationally-designed health initiatives with their local implementation.
Cubans call their system medicina general integral (MGI, comprehensive general medicine). Its programs focus on preventing people from getting diseases and treating them as rapidly as possible.
This has made Cuba extremely effective in control of everyday health issues. Having doctors’ offices in every neighborhood has brought the Cuban infant mortality rate below that of the US and less than half that of US Blacks.3 Cuba has a record unmatched in dealing with chronic and infectious diseases with amazingly limited resources. These include (with date eradicated): polio (1962), malaria (1967), neonatal tetanus (1972), diphtheria (1979), congenital rubella syndrome (1989), post-mumps meningitis (1989), measles (1993), rubella (1995), and TB meningitis (1997).4
The MGI integration of neighborhood doctors’ offices with area clinics and a national hospital system also means the country responds well to emergencies. It has the ability to evacuate entire cities during a hurricane largely because consultorio staff know everyone in their neighborhood and know who to call for help getting disabled residents out of harm’s way. At the time when New York City (roughly the same population as Cuba) had 43,000 cases of AIDS, Cuba had 200 AIDS patients.5 More recent emergencies such as outbreaks of dengue fever are quickly followed by national mobilizations.6
Perhaps the most amazing aspect of Cuban medicine is that, despite its being a poor country itself, Cuba has sent over 124,000 health care professionals to provide care to 154 countries.7 In addition to providing preventive medicine Cuba sends response teams following emergencies (such as earthquakes and hurricanes) and has over 20,000 students from other countries studying to be doctors at its Latin American School of Medicine in Havana (ELAM, Escuela Latinoamericana de Medicina).8
In a recent Monthly Review article, I gave in-depth descriptions of ELAM students participating in Cuban medical efforts in Haiti, Ghana, and Peru.9 What follows are 10 generalizations from Cuba’s extensive experience in developing medical science and sharing its approach with poor countries throughout the world. The concepts form the basis of the New Global Medicine and summarize what many authors have observed in dozens of articles and books.

Cuban-trained medical student examines Peruvian girl, Lima, Peru December 2010. Photo by Don Fitz.

Drs. María Concepción Paredes Huacoto & Johnny Carrillo Prada, Peruvian doctors trained in Cuba, by Consultorio No. 2 in Pisco, Peru, December 2010. Photo by Don Fitz.

Acupuncture is a part of Cuban medical training: Patient at Polyclinic of Natural and Traditional Medicine, Havana, Cuba, May 2012. Photo by Don Fitz.
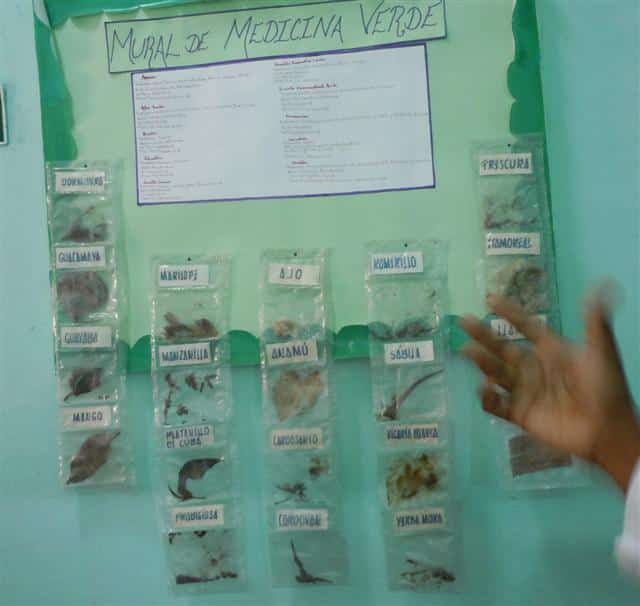
Use of herbs is a part of Cuban medical training: 4 Caminos University Polyclinic in rural area outside of Havana, Cuba, May 2012. Photo by Don Fitz.
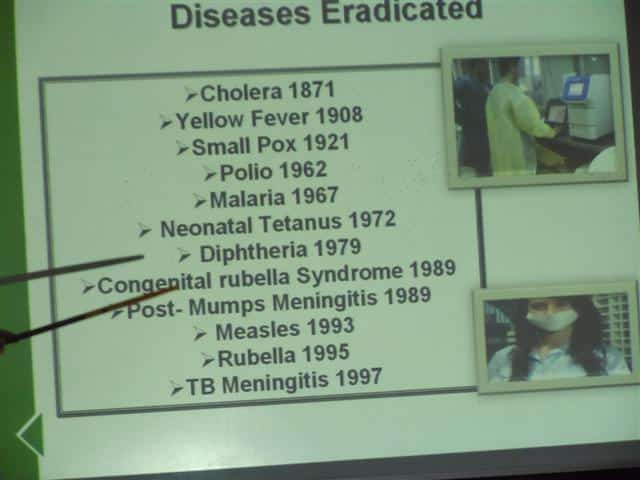
Cuba is a leader in eradicating diseases: Pedro Kouri Institute of Topical Medicine, Havana, Cuba, May 2012. Photo by Don Fitz.
Dan Hellinger Interviewed by Don Fitz, “Global Health Care: Venezuela” (Green Time, KNLC Channel 24, April 14, 2012)
https://www.youtube.com/watch?v=uJrOOHnOLRk
First, it is not necessary to focus on expensive technology as the initial approach to medical care. Cuban doctors use machines that are available, but they have an amazing ability to treat disaster victims with field surgery. They are very aware that most lives are saved through preventive medicine such as nutrition and hygiene and that traditional cultures have their own healing wisdom. This is in direct contrast to Western medicine, especially as is dominant in the US, which uses costly diagnostic and treatment techniques as the first approach and is contemptuous of natural and alternative approaches.
Second, doctors must be part of the communities where they are working. This could mean living in the same neighborhood as a Peruvian consultorio. It could mean living in a Venezuelan community that is much more violent than a Cuban one. Or it could mean living in emergency tents adjacent to where victims are housed as Cuban medical brigades did after the 2010 earthquake in Haiti. Or staying in a village guesthouse in Ghana. Cuban-trained doctors know their patients by knowing their patients’ communities. In this they differ sharply from US doctors, who receive zero training on how to assess homes of their patients.
Third, the MGI model outlines relationships between people that go beyond a set of facts. Instead of memorizing mountains of information unlikely to be used in community health, which US students must do to pass medical board exams, Cuban students learn what is necessary to relate to people in consultorios, polyclínicos, field hospitals, and remote villages. Far from being nuisance courses, studies in how people are bio-psycho-social beings are critical for the everyday practice of Cuban medicine.
Fourth, the MGI model is not static but is evolving and unique for each community. Western medicine searches for the correct pill for a given disease. In its rigid approach, a major reason for research is to discover a new pill after “side effects” of the first pill surface. Since traditional medicine is based on the culture where it has existed for centuries, the MGI model avoids the futility of seeking to impose a Western mindset on other societies.
Fifth, it is necessary to adapt medical aid to the political climate of the host country. This means using whatever resources the host government is able and willing to offer and living with restrictions. Those hosting a Cuban medical brigade may be friendly as in Venezuela and Ghana, be hostile as is the Brazilian Medical Association, become increasingly hostile as occurred after the 2009 coup in Honduras, or change from hostile to friendly as occurred in Peru with the 2011 election of Ollanta Humala. This is quite different from US medical aid which, like its food aid, is part of an overall effort to dominate the receiving country and push it into adopting a Western model.
Sixth, the MGI model creates the basis for dramatic health effects. Preventive community health training, a desire to understand traditional healers, the ability to respond quickly to emergencies, and an appreciation of political limitations give Cuban medical teams astounding success. During the first 18 months of Cuba’s work in Honduras following Hurricane Mitch, infant mortality dropped from 80.3 to 30.9 per 1,000 live births. When Cuban health professionals intervened in Gambia, malaria decreased from 600,000 cases in 2002 to 200,000 two years later. And Cuban-Venezuelan collaboration resulted in 1.5 million vision corrections by 2009. Kirk and Erisman conclude that “almost 2 million people throughout the world . . . owe their very lives to the availability of Cuban medical services.”10
Seventh, the New Global Medicine can become reality only if medical staff put healing above personal wealth. In Cuba, being a doctor, nurse, or support staff and going on a mission to another country is one of the most fulfilling activities a person can do. The program continues to find an increasing number of volunteers despite the low salaries that Cuban health professionals earn. There is definitely a minority of US doctors who focus their practice in low-income communities which have the greatest need. But there is no US political leadership which makes a concerted effort to get physicians to do anything other than follow the money.
Eighth, dedication to the New Global Medicine is now being transferred to the next generation. When students at Cuban schools learn to be doctors, dentists, or nurses their instructors tell them of their own participation in health brigades in Angola, Peru, Haiti, Honduras, and dozens of other countries. Venezuela has already developed its own approach of MIC (medicina integral comunitaria, comprehensive community medicine) which builds upon, but is distinct from, Cuban MGI.11 Many ELAM students who work in Ghana as the Yaa Asantewaa Brigade are from the US. They learn approaches of traditional healers so they can compliment Ghanaian techniques with Cuban medical knowledge.
Ninth, the Cuban model is remaking medicine across the globe. Though best-known for its successes in Latin America, Africa, and the Caribbean, Cuba has also provided assistance in Asia and the Pacific Islands. Cuba provided relief to the Ukraine after the 1986 Chernobyl meltdown, Sri Lanka following the 2004 tsunami, and Pakistan after its 2005 earthquake. Many of the countries hosting Cuban medical brigades are eager for them to help redesign their own health care systems. Rather than attempting to make expensive Western techniques available to everyone, the Cuban MGI model helps re-conceptualize how healing systems can meet the needs of a country’s poor.
Tenth, the New Global Medicine is a microcosm of how a few thousand revolutionaries can change the world. They do not need vast riches, expensive technology, or a massive increase in personal possessions to improve the quality of people’s lives. If dedicated to helping people while learning from those they help, they can prefigure a new world by carefully utilizing the resources in front of them. Such revolutionary activity helps show a world facing acute climate change that it can resolve many basic human needs without pouring more CO2 into the atmosphere.
----------
--------
Discussions of global health in the West typically bemoan the indisputable fact that poor countries still suffer from chronic and infectious diseases that rich countries have controlled for decades. International health organizations wring their hands over the high infant mortality rates and lack of resources to cope with natural disasters in much of the world.12
But they ignore the one health system that actually functions in a poor country, providing health care to all of its citizens as well as millions of others around the world. The conspiracy of silence surrounding the resounding success of Cuba’s health system proves the unconcern by those who piously claim to be the most concerned.
How should progressives respond to this feigned ignorance of a meaningful solution to global health problems? A rational response must begin with spreading the word of Cuba’s New Global Medicine through every source of alternative media available. The message needs to be: Good health care is not more expensive — revolutionary medicine is far more cost-effective than corporate-controlled medicine.
Notes
1 Don Fitz, “Eight Reasons US Healthcare Costs 96% More Than Cuba’s — With the Same Results,”AlterNet, December 9, 2010.
2 Lee T. Dresang, Laurie Brebrick, Danielle Murray, Ann Shallue, and Lisa Sullivan-Vedder, “Family Medicine in Cuba: Community-Oriented Primary Care and Complementary and Alternative Medicine,”Journal of the American Board of Family Medicine 18.4 (July-August 2005): 297-303.
3 Richard S Cooper, Joan F Kennelly, and Pedro Orduñez-Garcia, “Health in Cuba,”International Journal of Epidemiology 35 (2006): 817-824.
4 J. Pérez, “Gender and HIV Prevention,” Slide presentation at the Pedro Kouri Institute of Topical Medicine, Havana, Cuba, May 15, 2012.
5 Linda M. Whiteford and Laurence G. Branch, Primary Health Care in Cuba: The Other Revolution, Lanham: Rowman & Littlefield Publishers, Inc., 2008.
6 Don Fitz, “Med School Classes Cancelled in Havana,” Black Agenda Report, February 14, 2012,
7 John M. Kirk and H. Michael Erisman, Cuban Medical Internationalism: Origins, Evolution and Goals, New York: Palgrave Macmillan, 2009.
8 Don Fitz, “The Latin American School of Medicine Today: ELAM,” Monthly Review 62.10 (March 2011): 50-62.
9 Don Fitz, “Cuba: The New Global Medicine,” Monthly Review 64.4 (September 2012): 37-46.
10 Op. cit.
11 Steve Brouwer, Revolutionary Doctors: How Venezuela and Cuba Are Changing the World’s Conceptualization of Health Care. New York, Monthly Review Press, 2011.
12 Cooper, et al., op. cit.Don Fitz (fitzdon@aol.com) is editor ofSynthesis/Regeneration: A Magazine of Green Social Thought. He is Co-Coordinator of the Green Party of St. Louis and produces Green Time in conjunction with KNLC-TV 24.
Comments (0)
No comments:
Post a Comment